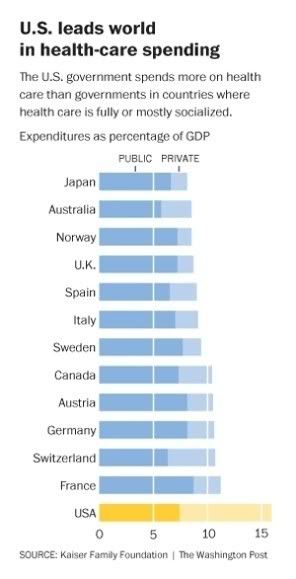
In the end, as Playwrite's graph indicates, publicly administered health care systems do a better job at containing health care costs than private systems, so if medicare can't provide effective health-care to the elderly that our society can afford, nothing will be able to.
What Samuelson's article glosses over is the difference between total health care costs and costs to individuals. What Ryan's plan does is replace the current medicare program where the elderly are provided a defined set of benefits with one where the elderly are given a set amount of money whose amount is indexed to inflation, not health care costs (which are rising faster than inflation, hence the "problem"). If the allowance doesn't cover the full expense of the procedure, and the patient can't pay for it out of pocket, then they don't get the care.
I love how Samuelson's argument against the CBO's projection that the Ryan plan will actually cause health care costs to be a third higher than under current version of medicare is just "Well, what if they're wrong"? I dunno Paul, what if they're wrong about the future deficits? Then we don't need to worry, do we? According to him we are supposed to take CBO reports at face value when they predict horrible deficits, but not when they predict something inconvenient to his argument.
He points to the fact that an earlier CBO prediction about the cost of the new medicare drug benefit was overestimated by 42 percent, and that the managed care plans in Medicare do not have higher cost than the fee for service plans under medicare that offer similar benefits, as evidence to support his argument that Ryan's plan will be able to cover more people, and hold down more costs than its critics say.
His second point is completely disingenuous because Medicare Advantage is structured completely differently than Ryan's plan. Under Medicare advantage, the private plans are required to offer a certain defined set of benefits, and, if medicare beneficiaries choose, they can opt for coverage under medicare that offers pretty much the same benefits. In effect, it a version of Obamacare with a very strong public option to hold down costs. The Ryan plan is completely different. There are no requirements as to what kind of benefits insurance companies need to offer, and no public option to hold down costs.
His first point is irrelevant since it is a short term evaluation of a CBO cost projection of a small component of overall health care in this country. Far more relevant would be to ignore the CBO entirely, and instead compare Ryan's plan with a similar "program" already in place - the private insurance market in the U.S. before the implementation of the Affordable Care Act.
According to Samuelson, with their new coupons from the government, elderly people are supposed to be somehow "empowered" to bargain with health insurance companies to lower prices. Its the magic market fairy again. If individuals now are not able to bargain with insurance companies in order to afford health care, why would the elderly suddenly be able to? If even large corporations can't use their size and bargaining power to control health care costs when they bargain for employee benefits, why would individual elderly people succeed where they fail?
Finally, the most galling part of Samuelson's article is that it ignores the fact that the Affordable Care Act already implements programs that move away from fee-for-service, which is what Samuelson bemoans as one of the primary causes of rising health causes, and what he says Ryan's plan is somehow supposed to address.
http://dpc.senate.gov/healthreformbill/healthbill25.pdf
In the end, health care is going to getting more expensive because more of it is available and a greater proportion of the population is getting older, so they will consume more health care. Publicly administered health care systems do a better job of containing costs than private systems, especially private systems that depend entirely on the "market" as a method of cost control. Still, we will most likely need to pay slightly more into medicare starting towards the end of the next decade absent drastic reforms such as the implementation of a medicare for all system.
I am willing to do that rather than abandon elderly people to a lack of care.